The Wolfram Syndrome
The Snow Foundation donation page
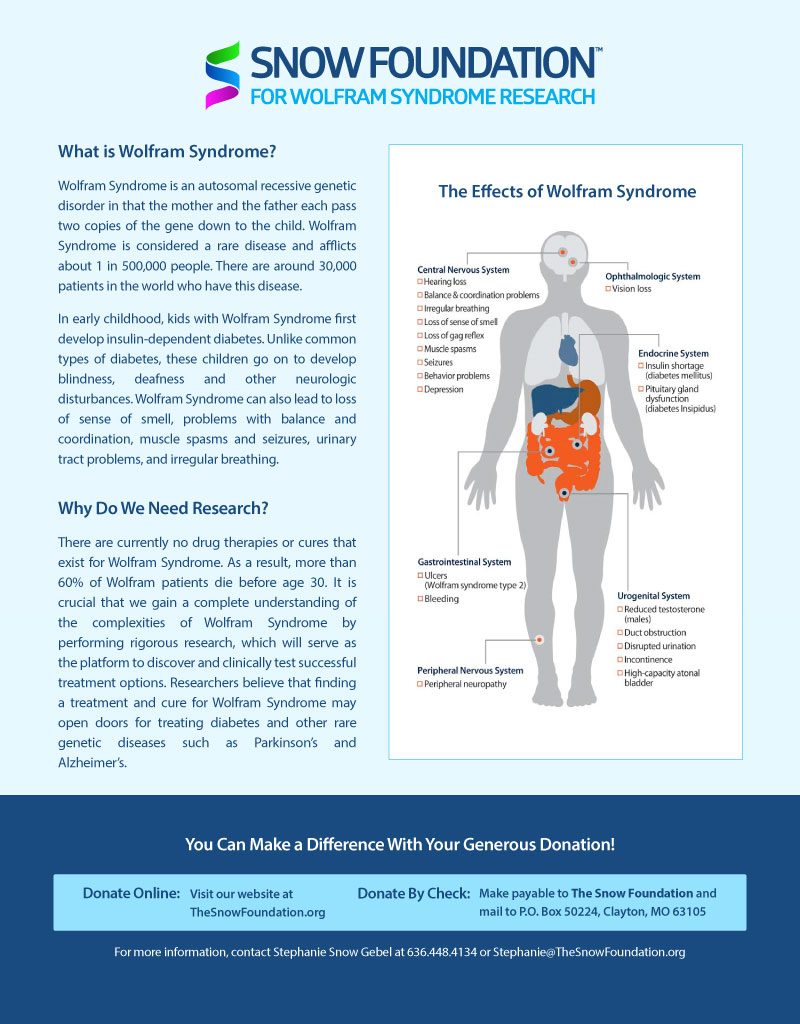
What is Wolfram Syndrome
Wolfram Syndrome is an autosomal recessive genetic disorder in that the mother and the father each pass two copies of the gene down to the child. Wolfram Syndrome is considered a rare disease and affects about 1 in 500,000 people. There are around 30,000 patients in the world who have this disease. In early childhood, kids with Wolfram Syndrome first develop insulin-dependent diabetes. Unlike common types of diabetes, these children go on to develop blindness, deafness and other neurologic disturbances. Wolfram Syndrome can also lead to loss of sense of smell, problems with balance and coordination, muscle spasms and seizures, urinary tract problems, and irregular breathing.
Why do we need research?
There are currently no drug therapies or cures that exist for Wolfram Syndrome. As a result, more than 60% of Wolfram patients die before age 30. It is crucial that we gain a complete understanding of the complexities of Wolfram Syndrome by performing rigorous research, which will serve as the platform to discover and clinically test successful treatment options. Researchers believe that finding a treatment and cure for Wolfram Syndrome may open doors for treating diabetes and other rare genetic diseases such as Parkinson’s and Alzheimer’s.
Are you or is someone you love affected?
The Symptoms of Wolfram Syndrome: “DIDMOAD”
Wolfram Syndrome (also known by its acronym, DIDMOAD*) is not an easy condition to diagnose. Most patients have it for years before the accurate diagnosis of Wolfram Syndrome (hereafter referred to as WS) is confirmed.
In non medical terms here are some of the complaints that you might have or see in your child
Type 1 Diabetes, usually starting between ages 5 and 15.
Unusually frequent urination in large volumes, combined with constant thirst. Bedwetting starts again long after successful night training.
Visual impairment, starting with wearing glasses, but rapidly increasing. You find yourself holding books of all kinds very close to your face.
Color blindness. Socks never match the outfit. The lawn has many patches of missed grass, after cutting. Color blindness in girls is very rare, except with WS patients.
Slow reacting iris in the eye. Even in bright light the pupils will never go pinpoint. This may not be obvious from a distance in people with brown eyes. This may be the first observable symptom in some cases.
High frequency hearing loss or tonal deafness becomes evident.
It is easy to become emotionally agitated or upset.
The challenge with these symptoms is that they are initially fairly mild. Any one of them is not unreasonable to overlook or treat as an individual anomaly.
If you find yourself or a family member with more than two of these symptoms please consult your family doctor immediately and refer them to the web links referenced here (print them off and take them in, might be the easiest way to insure that the doctor will at least take the time to look at them.)
This is a rare disease, don’t expect your physician to be well aware of its symptoms or solutions. You may be well advised to get a second opinion from an endocrinologist if your family doctor is not certain that you don’t have WS and you feel that the symptoms above describe you or your child.
While the initial symptoms of WS at the outset may not seem all that terrible, the secondary complications which are discussed in greater detail in the medical articles linked above certainly justify serious concern. WS is a progressive degenerative disease.
- DIDMOAD stands for Diabetes Insipidus, Diabetes Mellitus, Optical Atrophy, Deafness, thus the acronym. Some patients with WS will never display all four of its classic symptoms.
Patient Information Leaflet
Dr Timothy G Barrett
Senior Lecturer/Consultant Paediatrics
Department of Endocrinology
Birmingham Children’s Hospital
Steelhouse Lane
Birmingham B4 6NH – UK
February 7, 2000
What is Wolfram Syndrome (DIDMOAD)?
A syndrome is the name given to a condition where features occur in a consistent pattern, and where the cause is not understood. Wolfram syndrome is named after a Dr Wolfram, who in 1938 described 4 brothers and sisters from the same family with diabetes mellitus and optic atrophy. He worked in the Mayo Clinic in North America, and since then over 200 patients have been described in the world medical literature. It is also called DIDMOAD syndrome, after 4 common features (Diabetes Insipidus, Diabetes Mellitus, Optic Atrophy, and Deafness).
How common is it?
Wolfram syndrome affects about 1 in 770,000 of the total UK population, or 1 in 500,000 children, so it is very rare. A consultant paediatrician may only see one affected child in a professional lifetime.
What may happen in the condition?
Diabetes mellitus is the name given when the body cannot convert glucose or sugar to energy, because the pancreas is not making enough insulin hormone. Symptoms include thirst and frequent passing of urine, and weight loss. Glucose is passed out in the urine, and blood tests show a high level of glucose in the blood. This usually needs treatment with insulin injections for life.
Diabetes Insipidus is the name given when the body cannot concentrate the urine because the posterior pituitary gland in the head is not making enough vasopressin hormone. Symptoms again include thirst and frequent passing of urine. Urine tests show a very dilute urine. This can be treated by replacing the hormone with a nasal spray or tablets.
Deafness usually means difficulty in hearing in a crowded room, and difficulty hearing high pitched sounds. Some patients are helped with a hearing aid.
Optic atrophy means death of the optic nerve. Symptoms often present as difficulty seeing in the classroom at school, or everything going grey. There is no treatment for this.
Renal problems include loss of control over bladder function, so patients may wet the bed or have accidents. Some patients are helped by passing a tube or catheter, passed several times a day.
Neurological problems may occur; these may include loss of balance, sudden jerks of the muscles, depression, and breathing problems. Some of these problems may respond to drugs.
How do you tell if you have the condition?
Diabetes mellitus occurs in everyone on average at about 5 years of age. The latest onset of diabetes in this condition is about 16 years. Optic atrophy also occurs in everyone on average at about 10 years of age. The latest onset is about 19 years. If a young person does not have both these features by about 15 years, he is very unlikely to have Wolfram syndrome.
What is the outlook for a child with Wolfram syndrome?
The diabetes mellitus can be controlled with insulin injections. The vision problems usually, but not always, get worse, and often a patient will be registered blind within 8 years of diagnosis. About three quarters of patients get diabetes insipidus, and two thirds get deafness, in the teenage years. About two thirds get renal problems in their twenties. About the same proportion get neurological complications in their thirties. However, there may be a subgroup of patients who run a milder course and don’t get these additional complications. The oldest patient in the 1995 UK survey was 49 years.
What are the chances of having another affected child?
Wolfram syndrome is inherited as an autosomal recessive condition; this means that both parents carry one abnormal copy of the Wolfram gene, and one normal copy. For a child to be affected, he has to inherit two abnormal copies, one from each parent. The chances of parents having another affected child are about 25%. There is as yet no genetic test during pregnancy to tell if an unborn child is affected.
Will there be a cure for Wolfram syndrome?
Any cure is a long way off. The current research is to understand why mistakes in the Wolfram gene cause the syndrome. There are research groups in America, UK, Germany and Japan all investigating this problem. Wolfram syndrome research in the UK is being supported by Children Nationwide, and SPARKS.
Who can I go to for help?
There is a Wolfram syndrome website where you can register and contact other families affected all over the world (www.wolframsyndrome.org www.didmoad.org). It is also very important that you show this leaflet to your doctor so that he knows what information you have. If you have any questions about the information in this leaflet, please write to me and I will try and answer.
Current Research on Wolfram Syndrome
Research has officially started: to enroll we suggest you visit the
International Wolfram Syndrome Registry Website
Abstract: Wolfram Syndrome Research conducted by Washington University, St.Louis, Missouri, USA
General description
Wolfram syndrome is a genetic disorder that is frequently seen in affected individuals as juvenile onset diabetes mellitus and optic atrophy, along with diabetes insipidus and deafness. Most patients with this progressive, neurodegenerative disorder eventually develop all four symptoms and die prematurely. The form of diabetes seen in these patients is ‘insulin-dependent non-autoimmune diabetes mellitus’ and occurs at 6 years as the mean age of onset. When the pancreas from these individuals were examined, the islet cells were dying, and insulin producing (beta)-cells were selectively absent. This syndrome is inherited as autosomal recessive, implying that both the copies of the gene in any individual need to be defective to show the symptoms associated with this disease. It has also been noted that carriers of this syndrome, i.e. those who have only one defective copy of the gene, are estimated to represent 1% of the US population and are predisposed to psychiatric illness. While studying Wolfram’s patients from at least 3 different ethnic backgrounds, our laboratory has used linkage mapping and other genetic techniques to link a region of chromosome 4 to this syndrome. Further, we have isolated a gene from this region and found it to be defective in all Wolfram patients in our study. We have named this gene, Wfs-1.
Based on the observation that insulin producing (beta)-cells are absent in the affected individuals and on the initial molecular characterization of the Wfs-1 gene, we propose that the gene plays an important role in the survival of the (beta)-cells. To this end, we hope to first study the role of the gene in the development of diabetes in mice. Our strategy is to mutate the gene in mice and study the resulting phenotype. More specifically we are interested to see why a defect in the Wfs-1 gene renders the insulin producing cells, incapable of survival and thus assign a role for this gene in normal animals. We hope to apply this knowledge to the study of diabetes in humans. This gene can possibly be the target for new drugs developed to counter auto-immune diabetes mellitus, where progressive death of beta-cells is the primary cause of the disease. Further, the gene itself might represent a therapeutic agent for blocking the onset of diabetes by means of modern gene therapy procedures.
Scientific Abstract
Wolfram syndrome (WFS) was first described in 1938 as a combination of familial juvenile-onset diabetes mellitus and optic atrophy. Most patients with this progressive disorder die prematurely with widespread atrophic changes throughout the brain. Insulin-requiring diabetes mellitus occurs with mean age of onset at 6 years. When examined, pancreatic islets were atrophic and insulin-producing (beta)-cells selectively absent. The disease is believed to account for 1/150 patients with young-onset insulin-requiring diabetes mellitus. The pathogenesis of Wolfram syndrome is unknown. Linkage of the gene to markers on chromosome 4p was reported in 1994 and recently we were successful in the positional cloning of the WFS gene (WFS1). Comparison of the cDNA sequence of WFS1 with those in public databases revealed no related genes. This novel cDNA sequence codes for a polypeptide of 890 amino acid residues. Hydrophobicity analysis predicts the gene product to be a membrane protein.